Running research findings take considerable time to be passed down and reflected in the work of Physios, trainers, coaches and Runners. This is probably why so many of the comm
only held beliefs at this moment in time are best described as myths. I’m going to talk you through some of the most common myths that i hear in my practice as there are lots of recurring themes.
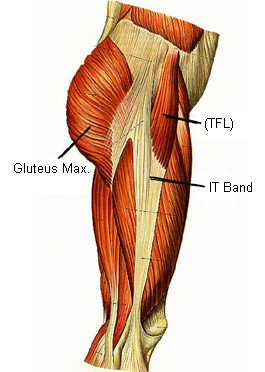
Running injury myth #1: You can stretch your ITB
The ITB is not a discrete structure, it is actually part of the fascia of the leg, which wraps around the entire leg like cling film. Fibers are thicker around the lateral side broducing a band-like structure that we refer to as the Illiotibial band (ITB). People like to talk about stretching their ITB’s but i’ll explain now why this is not really possible.
A study in 2010 looked at some of the most commonly prescribed ‘ITB stretches’ and found that they were actually stretching other things besides the ITB. Most often they were affecting the musculotendinous junction of tensor fascia late which runs from the iliac crest of the pelvis to the ITB.
Because the fascia is attached to the femur (thigh bone) the whole way down, there is absolutely no way that you can stretch it.
Because the fascia is attached to the femur (thingh bone) the whole way down, there is absolutely no way you can stretch it.

This won’t stretch your ITB
So the methods commonly prescribed to stretch the ITB don’t actually stretch it. It’s also questionable why you would actually want to stretch your ITB. It’s another common myth that the pain of illiotibial band syndrome (ITBS) which is usually felt to the outside of the knee, is caused by a ‘tight’ ITB. In fact it actually seems to, mot often, involve inflammation of a bursae underneath the ITB, resulting from compression– so nothing to do with ‘tightness’!
Pain in the region to the side of the knee is often referred to as illiotibial band syndrome (ITBS). In runners this can be caused by a combination of poor technique, poor gluteal control (on both the contra- and ipsilateral side) and repetitive mileage.
Treatments targeting the tensor fascia late (TFL) muscle which sits behind your front trouser pocket, at the top of the ITB, may be able to affect musculotendinous tension to the lateral leg.
However, i see deep tissue massage and foam rolling to the lateral thigh being more commonly prescribed, usually with the goal of stretching or loosening the ITB. These can’t possibly affect things as all you’re doing is compressing the fascia against the muscle. Don’t worry, foam rolling does have it’s uses…it just won’t stretch, elongate, or loosen your ITB.
Foam rolling the side of your thigh is probably an unnecessary form of self-torture!
If we consider that the symptoms of ITBS often involve compression of the bursae, then a treatment modality such as foam rolling or deep tissue massage, which causes even more compression, doesn’t make much sense. And remember, ITB pain is not caused by your ITB being ‘Tight’…so you can stop worrying about trying to stretch it.

This won’t stretch your ITB
I see a lot of runners (especially females) who get tender around the attachment sites at the Illiac crest, likely due to fatigue produced by stabilising the pelvis during running. Poor stabilisation, technique errors and general weakness in Quadratus Lumborum, Glute Med, Glute Min and Glute Max could all be contributing to this phenomena. Any big stretch that stresses attachment sites that are already sensitive can cause problems, especially when it uses a long lever like the ‘ITB stretch’ shown here. I remember one elite track athlete i worked with who had injured herself by doing the commonly prescribed ‘ITB stretch’ shown above, after a tough session of 400m repeats. Incidentally, i never prescribe forceful stretches to be performed at the end of tough training sessions.
A detailed history revealed that she had been suffering with on-going, low grade tenderness along the iliac crest. The stretch for her was likely the ‘straw that broke the camels back’ and overly stressed the already sore (and possibly degenerate) attachment sites. This particular ‘ITB stretch’ could be likened to a deep ankle/soleus stretch that stresses the insertional portion of the Achilles. This is probably fine in an asymptomatic Achilles, but if you have insertional Achilles tendinopathy, this stretch can really stir things up.
I don’t propose to know everything… just to get you thinking.
As ever, if you have ongoing symptoms, get them checked out by a Physiotherapist or Sports Doctor in your area.
